Number 28 (Replaces Practice Advisory: Updated Cervical Cancer Screening Guidelines, April 2021)
This Committee Statement was developed by the American College of Obstetricians & Gynecologists' Committee on Clinical Consensus–Gynecology in collaboration with Christopher Zahn, MD, Akiva P. Novetsky, MD, MS, Kimberly Gecsi, MD, and Nancy Sokkary, MD.
ASCCP and the Society of Gynecologic Oncology endorse this Committee Statement.
ABSTRACT: This committee statement announces the American College of Obstetricians & Gynecologists’ qualified endorsement of the 2026 Women's Preventive Services Initiative's (WPSI) updated cervical cancer screening guidelines and addresses cervical cancer screening for patients at average risk in the following age categories: 21–29 years, 30–65 years, and older than 65 years. This committee statement discusses specific qualifications to the WPSI guidelines, particularly regarding self-collection for primary high-risk human papillomavirus screening, among other implementation considerations.
Summary of Recommendations
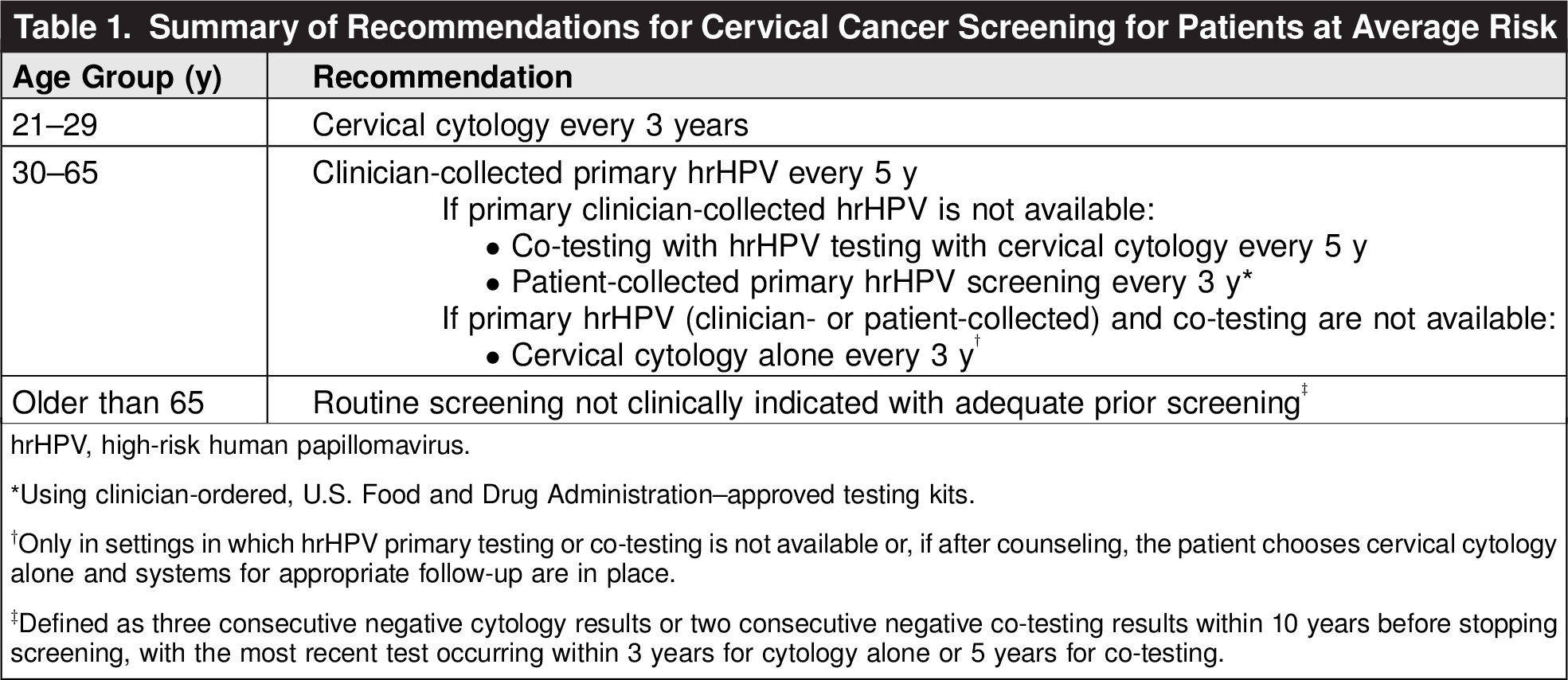
The American College of Obstetricians & Gynecologists (ACOG) endorses the Women's Preventive Services Initiative’s (WPSI) updated cervical cancer screening recommendations for patients at average risk Table 1 ):
Individuals aged 21–29 years should be screened for cervical cancer every 3 years with cervical cytology alone.
Individuals aged 30–65 years should undergo clinician-collected primary high-risk human papillomavirus (hrHPV) screening every 5 years, using U.S. Food and Drug Administration–approved tests for primary screening.
Co-testing with hrHPV and cervical cytology every 5 years for individuals aged 30–65 years is acceptable when primary hrHPV testing is not available or, after counseling, the patient chooses co-testing. Patient-collected primary hrHPV screening every 3 years, using U.S. Food and Drug Administration–approved testing kits, may be considered when systems are in place for appropriate notification and follow-up.
Cervical cytology alone for individuals aged 30–65 years should be used only in settings in which primary hrHPV testing or co-testing is not available or if, after counseling, the patient chooses cervical cytology alone.
Routine screening is not clinically indicated in patients older than age 65 years if they have received adequate prior screening, defined as three consecutive negative cytology results or two consecutive negative co-testing results within 10 years before stopping screening, with the most recent test occurring within 3 years for cytology alone or 5 years if co-testing is used. For patients older than age 65 years who have not received adequate prior screening according to the criteria described or who are at high-risk for cervical cancer, screening should continue.
Routine cervical cancer screening is not recommended for patients who have undergone hysterectomy with removal of the cervix and who do not have a history of cervical cancer or another high-grade precancerous lesion.

Background
ACOG has updated its cervical cancer screening recommendations based on the 2026 update to the WPSI cervical cancer screening recommendations, adopted by the HRSA 2 3 4.
These recommendations do not apply to patients with human immunodeficiency virus (HIV), immunocompromised patients without HIV, and patients with in-utero diethylstilbesterol (DES) exposure For patients aged 21–29 years, those older than age 65 years, and those who have undergone hysterectomy with removal of the cervix, ACOG's screening recommendations, as listed above, remain unchanged and align with the WPSI screening recommendations. ACOG also recognizes that the American Cancer Society (ACS) includes primary hrHPV screening as an option for patients aged 25–29 years 5. In addition, ACOG recognizes that the ACS has amended its 2020 cervical cancer screening guideline for stopping screening, incorporating primary hrHPV testing, co-testing, or cytology performed at specific ages, before considering stopping screening 6. For patients aged 30–65 years, the WPSI recommendations include screening with clinician-collected hrHPV primary screening as the preferred option. Alternative options include co-testing (using a combination of hrHPV testing with cervical cytology) or continued cervical cytology screening alone. ACOG's recommendations, although similar, provide qualifications to these recommendations based primarily on implementation concerns. Prior ACOG recommendations included clinician-collected hrHPV primary screening or co-testing every 5 years or cervical cytology alone every 3 years as essentially equivalent options. Based on the evidence supporting the WPSI recommendations, the draft evidence review performed for the U.S. Preventive Services Task Force, and the expanding availability of hrHPV primary screening, ACOG currently considers clinician-collected hrHPV primary screening as the preferred option, with co-testing as an acceptable alternative 7 7. ACOG also recognizes that the ACS has updated their cervical cancer screening recommendations to include hrHPV patient collection as an option 6. It is important to note that much of the evidence on self-collection (ie, patient collection) is from non-U.S. settings and involves patient-collected samples outside of the clinician office environment. The currently available patient-collected hrHPV tests are approved solely for samples ordered or approved by a clinician for patients aged 25–65 years. If self-collection is used, only U.S. Food and Drug Administration–approved, clinician-ordered, or clinician-approved test kits should be used. ACOG acknowledges that patient-collected hrHPV sampling can extend screening to patients who might not otherwise be screened. However, it is critical that appropriate policies and processes be in place for documentation, notification, and follow up as indicated based on test results before health care settings or health care professionals offer patient-collected testing. If those systems are not fully established, patient-collected sampling could lead to missed diagnoses and errors, which could be magnified if the patient is not screened again for another 3–5 years. As a result, patient-collected primary hrHPV screening should be performed only if patients prefer this collection method and when notification, documentation, and follow-up processes are in place. A further consideration related to patient-collected hrHPV primary screening is the recommended time interval. Data supporting a 5-year interval are lacking; available data support 3-year screening intervals 9. ACOG therefore recommends that, if patient-collected hrHPV primary screening is used, 3-year intervals are followed until there is sufficient evidence to support a 5-year screening cadence. Additionally, it is important to recognize clinical situations for which neither clinician-collected nor patient-collected hrHPV testing alone is recommended, including cervical cancer screening in people with HIV, screening for patients with in-utero DES exposure, surveillance after colposcopy for atypical glandular cells in which no cervical intraepithelial neoplasia 2+ is identified, and surveillance after the diagnosis of adenocarcinoma in situ has been made 9. An additional concern with patient-collected sampling is the potential for overscreening, including screening performed more frequently than the recommended interval as well as screening outside of the recommended age ranges. These results and interpretations will pose a challenge, because they may be outside any accepted protocol for screening; therefore, interventions and follow-up recommendations are not known. For that reason, ACOG strongly recommends that patient collection should be performed only under a clinician-guided process or with a clinical infrastructure in place. Guidance for further evaluation or management in these situations will be needed, as well as the notification, documentation, and follow-up processes as previously described. It is also critically important to recognize the potential effect of these recommended screening strategies on access and health equity. Patients in underserved communities experience lower rates of cervical cancer screening and higher rates of cervical cancer incidence and mortality 10 11 12. The goal of preventive care is to maximize the opportunity for screening all eligible individuals; it is essential that underserved populations are not limited to screening options that potentially worsen disparities. Patient-collected hrHPV primary screening may increase screening, but ensuring that all patients have opportunities for appropriate counseling and follow up is critical.Rationale and Implementation Considerations
Conclusion
In summary, ACOG endorses the current HRSA–WPSI updated cervical cancer screening guidelines, but with qualifications as listed. Although there may be slight differences between the ACOG recommendations and the WPSI recommendations, the most significant overarching principle is to maximize the opportunity for and access to screening. Underscreening, or no screening, is the most significant contributor to the development of cervical cancer. Continued efforts to have screening available and accessible to all eligible patients are warranted.
Use of Language
The American College of Obstetricians & Gynecologists recognizes and supports the gender diversity of all patients who seek obstetric and gynecologic care. In this document, authors seek to use gender-inclusive language or gender-neutral language. When describing research findings, this document uses gender terminology reported by investigators. To review ACOG's policy on inclusive language, see Inclusive Language (https://www.acog.org/clinical-information/policy-and-position-statements/statements-of-policy/2022/inclusive-language).
Conflict of Interest Statement
All ACOG committee members and authors have submitted a conflict-of-interest disclosure statement related to this published product. Any potential conflicts have been considered and managed in accordance with ACOG’s Conflict of Interest Disclosure Policy. The ACOG policies can be found on acog.org . For products jointly developed with other organizations, conflict of interest disclosures by representatives of the other organizations are addressed by those organizations. The American College of Obstetricians & Gynecologists has neither solicited nor accepted any commercial involvement in the development of the content of this published product.