Number 30 July 2026
This Committee Statement was developed by the American College of Obstetricians & Gynecologists' Committee on Advancing Equity in Obstetric and Gynecologic Health Care in collaboration with Lisa Nathan, MD, MPH, and Maria Small, MD, MPH.
ABSTRACT: In the United States and globally, the negative effects of climate change, such as extremes of heat, wildfire smoke, and air pollution, are associated with early pregnancy loss, preterm birth, preeclampsia, hypertensive disorders of pregnancy, and stillbirth. Climate change amplifies existing gender-based disparities, which include elevated risks of infectious diseases, malnutrition, sexual violence, mental health disorders, lack of reproductive control, negative obstetric outcomes, and death, when compared with men. These adverse effects disproportionately affect marginalized groups. With the ongoing and increasing threats of climate change and environmental pollutants on human health, it is imperative that obstetrician–gynecologists (ob-gyns) educate not only themselves but students, other health care professionals, their patients, and communities about the adverse effects these threats have on gynecologic and obstetric health. Institutions should encourage the inclusion of climate change education in medical curricula. Ob-gyns should incorporate environmental health education into all prepregnancy counseling visits, with a focus on identifying any potential harmful exposures and determining what mitigation efforts can be initiated before pregnancy.
Summary of Recommendations and Conclusions
Based on the principles outlined in this Committee Statement, the American College of Obstetricians & Gynecologists (ACOG) recommends that obstetrician–gynecologists (ob-gyns) do the following:
Support policies that promote equitable and healthy built environments for all people.
Educate ob-gyn colleagues, medical students, other health care professionals, patients, and communities about the adverse effects of climate change and related environmental exposures on individuals seeking obstetric and gynecologic care.
Support and advocate for research on the effects of climate change and climate-related environmental exposures on individuals seeking obstetric and gynecologic care; special attention should be devoted to understanding the effects on specific communities, such as minoritized or socioeconomically marginalized communities. These initiatives should identify actionable interventions, policies, and solutions that promote climate resilience.
Support policies to be inclusive of the health of patients with time-sensitive obstetric and gynecologic needs in the setting of natural disasters.
Support and advocate for environmentally responsible practices in health care institutions.
Background
The term climate change often is used interchangeably with global warming. Climate change, however, refers specifically to the shifts in average temperature seen over periods of time, resulting in long-term changes in weather patterns and climate systems 4. These differences are rooted in physiology, as well as women's social, cultural, and socioeconomic roles. Climate change amplifies existing gender-based disparities, which include elevated risks of infectious diseases, malnutrition, sexual violence, mental health disorders, lack of reproductive control, negative obstetric outcomes, and death, when compared with men 5. Due to the many physiologic changes of pregnancy, pregnant individuals are highly vulnerable to the effects of climate change 6. In particular, pregnant individuals’ increase in oxygen consumption, minute ventilation, and cardiac output places them at unique risk of the effects of excess heat and air pollution 7. In the United States and globally, the negative effects of climate change, such as extremes of heat, wildfire smoke, and air pollution, are associated with early pregnancy loss, preterm birth, preeclampsia, hypertensive disorders of pregnancy, and stillbirth 8 9. These adverse effects disproportionately affect marginalized groups 8 10.
Health inequities are intertwined with underlying social inequities, including systematic racial inequities and poverty, and the effects of climate change are not experienced equally among individuals, communities, and societies 11 12. Black, Indigenous, and people of color are more likely to reside in areas with higher heat and air pollution exposure 11. According to the EPA, Black individuals are approximately 40% more likely to reside in areas with the highest projected heat-related deaths when compared with non-Black individuals and are 34% more likely to currently live in areas with the highest projected increases in childhood asthma diagnoses. Hispanic and Latino individuals are approximately 43% more likely than non-Hispanic and non-Latino individuals to live in areas with the highest loss of labor hours due to extreme temperatures 10 14. The social movement of environmental justice, which seeks to address the effects of racism on environmental health outcomes, began in the 1980s in response to toxic waste disposal in predominately Black communities 14 15 16 17. This movement, as well as the climate justice movement, addresses the disparate health effects of climate change on marginalized communities. See Box 1 for definitions of environmental terms.
Box 1.
Definitions
Adaptive capacity : The ability of a human or natural system to adjust to climate change (including climate variability and extremes) by moderating potential damages, taking advantage of opportunities, or coping with the consequences.*
Built environment: The human-made or modified structures that provide people with living, working, and recreational spaces, including buildings; distribution systems that provide water and electricity; and roads, bridges, and transportation systems.†
Climate adaptation : Taking action to prepare for and adjust to both the current and projected effects of climate change.‡
Climate change : A change in the state of the climate that can be identified (eg, by using statistical tests) by changes in the mean or variability of its properties, or both, and that persists for an extended period, typically decades or longer. Climate change may be due to natural internal processes or external forces such as modulations of the solar cycles, volcanic eruptions, and persistent anthropogenic changes in the composition of the atmosphere or in land use.§
Climate mitigation: Actions limiting the magnitude and rate of future climate change by reducing greenhouse gas emissions.‡
Climate resilience: The capacity of a system to maintain function in the face of stresses imposed by climate change and to adapt the system to be better prepared for future climate effects.‡
Environmental justice: The concept that all people—regardless of race, color, national origin, or income—are entitled to equal protection from environmental and health hazards and equal access to the development, implementation, and enforcement of environmental laws, regulations, and policies.‡
Environmental racism: The disproportionate effects of environmental hazards (eg, pollution, toxic waste disposal, industrial activities) on Black, Latino, and Indigenous communities and populations with low-income. It is a form of systemic racism that results in these marginalized groups bearing an unequal burden of environmental health risks and degraded living conditions.||
Environmental sustainability: To create and maintain conditions under which humans and nature can exist in productive harmony that permit fulfilling the social, economic, and other requirements of present and future generations.¶
Redlining: A discriminatory practice that consists of the systematic denial of services such as mortgages, insurance loans, and other financial services to residents of certain areas based on their race or ethnicity.#
*U.S. Environmental Protection Agency. U.S. Environmental Protection Agency climate adaptation action plan. Accessed February 23, 2026. https://www.epa.gov/system/files/documents/2021-09/epa-climate-adaptation-plan-pdf-version.pdf
†U.S. Environmental Protection Agency. Basic information about the built environment. Accessed February 23, 2026. https://www.epa.gov/smm/basic-information-about-built-environment#builtenviron
‡Centers for Disease Control and Prevention. Centers for Disease Control and Prevention Agency-wide Climate and Health Task Force FY 2022 strategic framework. Accessed February 23, 2026. https://www.cdc.gov/climate-health/media/pdfs/2024/06/Agency-Climate-Health-External-Strategic-Framework-508.pdf
§Field CB, Barros VR, Dokken DJ, Mach KJ, Mastrandrea MD, Bilir TE, et al, editors. Climate change 2014: impacts, adaptation, and vulnerability. Part a: global and sectoral aspects. Working Group II contribution to the fifth assessment report of the Intergovernmental Panel on Climate Change. Intergovernmental Panel on Climate Change; 2014. Accessed February 23, 2026. https://www.ipcc.ch/report/ar5/wg2/
||UMass Chan Medical School, Lamar Soutter Library. Environmental racism: what it is and connection to redlining in the United States. Accessed March 17, 2026. https://libraryguides.umassmed.edu/EnvironmentalJustice/racism
¶National Research Council. Sustainability and the U.S. EPA. Accessed February 23, 2026. https://www.nationalacademies.org/projects/PGA-STS-10-04/publication/13152
#Legal Information Institute. Redlining. LII; 2022. Accessed February 23, 2026. https://www.law.cornell.edu/wex/redlining
Recommendations and Conclusions
Support policies that promote equitable and healthy built environments for all people.
The built environment describes human-made structures such as parks, roads, sidewalks, and buildings that form part of the neighborhoods and communities where people live, work, and socially engage 18. Historically, minoritized communities have been affected by broad social disinvestment in infrastructure (eg, greenspace, tree-canopy coverage, housing stock, and roads) and services (eg, schools, garbage collection), creating social disadvantages and disparate health outcomes 19. Although greenspaces, considered a protective barrier from environmental harms, are associated with positive health outcomes, such as lower risk for preterm birth and premature mortality 20, the history of residential segregation has resulted in reduced greenspace in Black and poor communities 21. There is a demonstrated association between historical “redlining,” or the discriminatory mortgage appraisal practice of banks and insurers, and access to greenspaces through measures of the Normalized Difference Vegetation Index values 21. Redlining intensified existing residential segregation after the 1930s federal regulation for city map development that reflected investment security risks. The maps, created through the Home Owners' Loan Corporation, were designed to improve homeownership after the Great Depression 19. Developed as part of the New Deal to systematize investment risk, these maps included items such as prior home values and racial composition. Neighborhoods were graded, then shaded and outlined in four colors; green was “good,” whereas red was “hazardous” and deemed to be at the highest risk 22. Redlines and red shading were placed predominately in Black communities, as well as in communities with populations of Jewish, Asian, Hispanic, and immigrant individuals 22 23. Home Owners' Loan Corporation workers applied terms such as “infiltration” and “foreign-born” to these areas. Residents in redlined areas could not receive Home Owners' Loan Corporation loans; therefore, Black homebuyers received more predatory loans and many were deprived of home ownership altogether, a primary source of familial wealth generation and transfer. Additionally, restrictive covenants, such as those barring Black residents from White neighborhoods, also supported violence against Black individuals who chose to enter these communities or groups that chose to form integrated co-ops or communities 19.
Today, data demonstrate a clear association between those communities that were historically redlined and increased climate vulnerability, especially negative health outcomes related to heat 23. Redlined maps and satellite imagery demonstrate an association between the legacy of this discriminatory policy and environmental health outcomes, such as the likelihood of tree canopy and other mitigators of air pollution and heat 22 24. Patterns of racial discrimination and persistent segregation determine which neighborhoods have access to ecologic benefits (eg, parks, greenspace, tree canopy, vegetative cover), and formerly redlined areas are associated with higher rates of poverty, higher land surface temperatures, and lower vegetative cover when compared with areas that were not redlined 25. Neighborhoods that historically were redlined currently are disproportionately affected by adverse health outcomes, including higher prevalences of cancer, asthma, poor mental health, and lack of health insurance 26. Both extreme heat and flooding are linked with an increased risk of adverse pregnancy and birth outcomes, including preeclampsia and low birth weight 27. Additionally, Black and Hispanic individuals are more likely than White individuals to live in communities disproportionately exposed to air pollution; they also experience higher rates of adverse health effects from air pollution due to higher rates of preexisting comorbidities (eg, asthma, diabetes, cardiovascular disease) 7 Box 2 for resources to assist health care professionals in attaining a foundational understanding of environmental health and climate change and evidence-based suggestions on how to effectively communicate about these issues.
Box 2.
Educational Resources and Tools for Health Care Professionals*
Climate Change and Human Health Extension for Community Healthcare Outcomes (ECHO)
Climate ECHO is a program that engages health professionals to discuss climate-related issues with patients. The tele-mentoring program aims to improve climate literacy and climate change‒related communication skills for health care professionals and to build resources and capacity.†
The Centers for Disease Control and Prevention's Climate and Health Resources
These resources for public health professionals include webinars on important climate and health topics, guidance documents, toolkits, and other materials to use in climate adaptation planning and implementation.
This toolkit aims to help health professionals effectively communicate about climate change and health.
The Center for Climate, Health, and the Global Environment
• Climate Communication: 10 Research-backed Tips
Evidence-based tips to help clinicians be more effective when talking with patients or the public about the health effects of climate change.
• Climate Resilience for Frontline Clinics Toolkit
The toolkit provides resources for health care professionals, patients, and clinic administrators to meet the health care challenges of climate change. As climate-related health threats become more severe, this toolkit is helping frontline clinics improve their disaster resilience and improve health outcomes for their patients. Resources include clinical guidance, tip sheets and action plans for patients, checklists for clinic staff, and materials to protect patients with certain health conditions from extreme heat.
Health Care Without Harm's Physician Network
As trusted voices in their communities, health professionals have a unique opportunity to advance sustainable, climate-smart health care. The Physician Network, part of the Climate-Smart Collective, supports members in leveraging their influence and expertise to advance the growing health care sustainability movement and create climate-smart health care.
*The following resources are for information purposes only. Referral to these sources and websites does not imply the endorsement of the American College of Obstetricians & Gynecologists. These resources are not meant to be comprehensive. The exclusion of a source or website does not reflect the quality of that source or website. Please note that websites are subject to change without notice.
†For more information, see Katzman JG, Balbus J, Herring D, Bole A, Buttke D, Schramm P. Clinician education on climate change and health: virtual learning community models. Lancet Planet Health 2023;7:e444–6. doi: 10.1016/S2542-5196(2300087-6).
Ob-gyns should be aware of the effects of rising temperatures and environmental changes on reproductive health. For example, increased exposure to pollutants, ultraviolet radiation, and endocrine-disrupting chemicals is associated with a higher incidence of breast, ovarian, and cervical cancers 29. Additionally, climate change–related natural disasters (eg, hurricanes, flooding) lead to the disruption of health care services and limit timely screening and diagnosis of cancer 29. As reported by patients with gynecologic cancer who lived in areas affected by catastrophic Hurricanes Irma and Maria, climate crises result in major disruptions in essential services (eg, the availability of potable water and electric power, telecommunications, transportation) and environmental health issues (eg, extreme heat, water sanitation, contaminant exposure, vector-borne diseases, food hygiene, carbon monoxide poisoning, and mold exposure), affecting patients' well-being 30. Although data are limited, researchers have found an association between the effects of climate change (eg, extreme temperatures, wildfires) and female infertility 31 32 and disaster-related increases in exposure to endocrine-disrupting chemicals and earlier age at menopause 33.
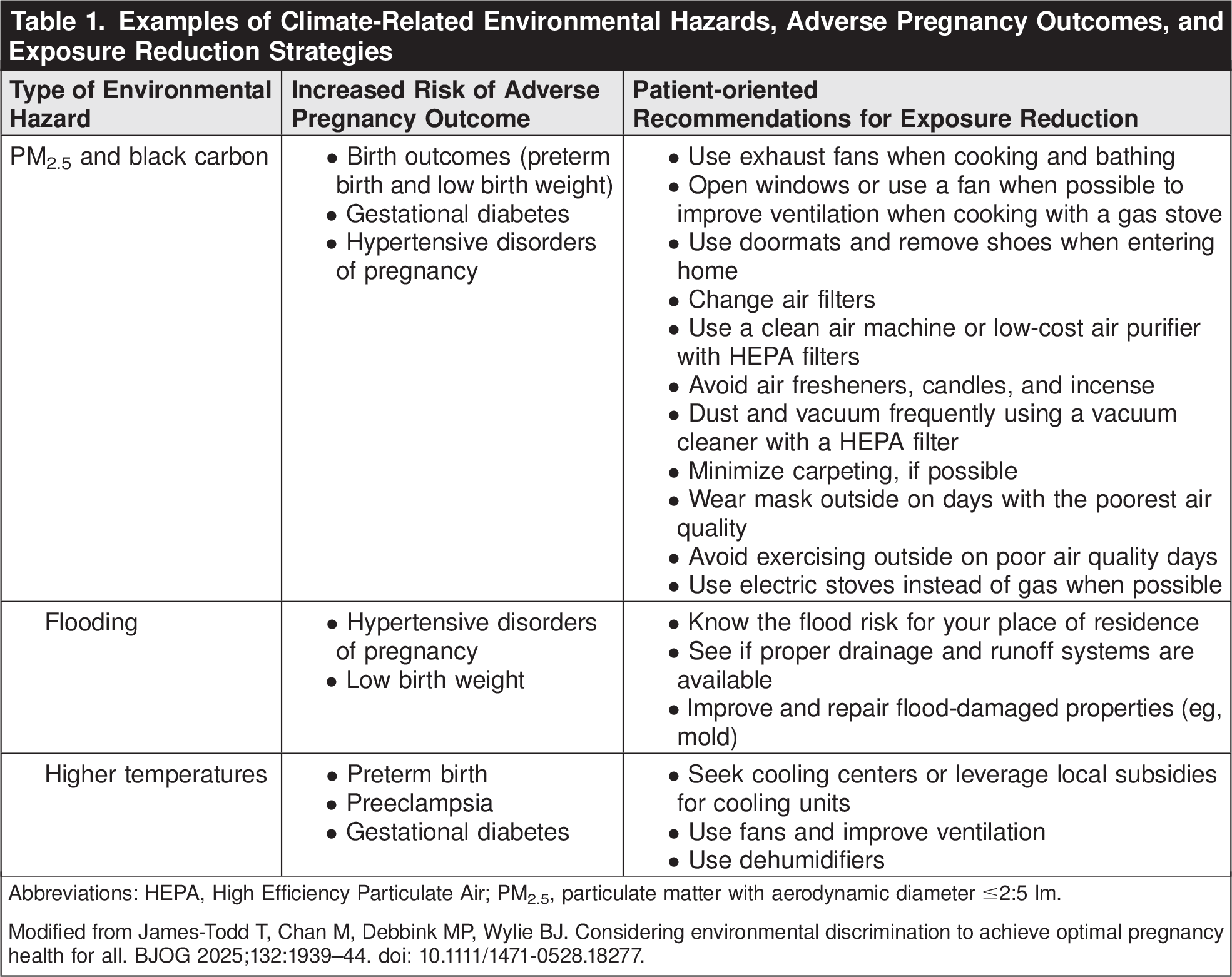
Ob-gyns should incorporate environmental health education into all prepregnancy counseling visits, with a focus on identifying any potential harmful exposures and determining what mitigation efforts can be initiated before pregnancy 34. Exposure to a wide range of pollutants and extreme climates may result in early pregnancy loss, congenital anomalies, developmental abnormalities, growth restriction, preeclampsia, stillbirth, preterm birth, gestational diabetes, and mental health concerns 8 9. See Table 1 for examples of environmental hazards, adverse pregnancy outcomes, and exposure-reduction strategies. Ongoing prenatal care should include the repeated evaluation of prenatal patients' exposure to the harmful effects of climate change and toxic environmental pollutants 35.

Support and advocate for research on the effects of climate change and climate-related environmental exposures on individuals seeking obstetric and gynecologic care; special attention should be devoted to understanding the effects on specific communities, such as minoritized or socioeconomically marginalized communities. These initiatives should identify actionable interventions, policies, and solutions that promote climate resilience.
In the United States, structural racism—the ways in which institutions, policies, and processes both create and fortify discriminatory practices and inequities among racial and ethnic groups—is a long-standing contributor to environmental health inequities and injustices 12 36. These patterns and practices in turn reinforce discriminatory beliefs, values, and distribution of resources 37. These structural, systemic foundations inform how individuals and communities respond to and are affected by environmental exposures and climate change. Data are needed to develop effective, evidence-based solutions to the ongoing effects of climate change on disproportionately affected communities. Investigators should use a racial justice lens when developing research strategies 38. As detailed by the National Academies of Sciences, Engineering, and Medicine, research should partner with those communities most affected by climate change, with a focus on building trust and engagement, and research projects themselves should include researchers from those populations most at risk 26 40, the effects of extreme heat on minoritized laborers 41. Due to rapid environmental changes, continued research is essential to monitor health effects and develop effective policy and public health solutions and interventions 42.
The federal government plays an essential role in funding research, as well as in the implementation of policies and programs; it should prioritize research, policies, and programs on the effects of climate change on health outcomes. Past work by the EPA, the Centers for Disease Control and Prevention, and the National Institutes of Health provide important roadmaps to address climate change 44. Government researchers and policy makers also play an essential role in furthering the understanding of the effects of climate change on health. Existing data on environmental health, racism, and justice developed by government programs and agencies should be protected, and this critical scientific evidence should be freely available to health care professionals and the public. Removing or limiting access to data and information does not constitute good health policy or contribute to improved health outcomes. ACOG supports federal efforts to address the health effects of climate change, including federal funding for the Centers for Disease Control and Prevention's National Center for Environmental Health 4 46 47. For more information on emergency planning, see ACOG's Committee Statement No. 15, Preparing for Disasters: Addressing Critical Obstetric and Gynecologic Needs of Patients 48. See Box 3 for guidance on returning to areas affected by disasters.
Box 3.
Standards to be Met for Pregnant Individuals and Families to Return to Areas Affected by Disasters
Functional utilities and public services
Reestablished water supply for drinking and bathing must meet applicable existing standards for biological, chemical, and mineral contaminants
Restored electricity and gas and repair of damage to transmission system or gas pipes
Reestablishment of reliable food supply with available and appropriate food storage
Functional sanitation system, including sewage
Debris collection and regular trash collection
Functional, reliable, and readily accessible emergency services and communication system, including 9-1-1 access
Available and accessible health care services, including mental health services
Readily accessible medications and medical supplies
Areas cleaned and made safe, including from mold
Knowledge of the location of nearest functioning hospital providing obstetric care and route to reach hospital
Natural disasters, such as heat waves, do not affect all populations equally, and higher risk of health-related death is associated with factors such as age, sex, education, and neighborhood socioeconomic status 49. Numerous studies demonstrate that Black, Latinx, and Native American individuals in the United States are at increased risk of heat-related mortality when compared with White individuals 50. Incarcerated individuals also are at increased risk of adverse physical, mental, and behavioral outcomes during times of extreme temperatures 49. Data on the Heat Action Model Plan demonstrated some overall mortality reduction, with the greatest effects found in programs for the elderly and populations living in low socioeconomic neighborhoods 49.
Support and advocate for environmentally responsible practices in health care institutions.
In addition to understanding the effect of climate change on reproductive health care, ob-gyns should understand the role health care itself plays in contributing to environmental changes. As in other systems, the provision of health care creates environmental waste. Health care professionals and institutions can strive to be good community partners and should work to minimize the environmental effect of their work. Health care–related emissions of greenhouse gases are a worldwide problem, accounting for 4–10% of global greenhouse emissions, generally attributable to the use of energy, anesthetic gases, and disposable items 9 53. Within the United States, the health care sector is responsible for 10% of the country's total greenhouse gas emissions 9. Many of the inhaled anesthetic gases used in gynecologic surgery, such as nitrous oxide, isoflurane, desflurane, and sevoflurane, are markedly potent greenhouse gases and have from 350 up to 3,700 times the global warming potential of an equivalent amount of carbon dioxide 9 54. Minor institutional changes potentially can make a major difference. For example, switching from the central delivery of nitrous oxide to point-of-care nitrous oxide cylinders can minimize emissions of a potent greenhouse gas into the environment 55. Although there are many important clinical factors to consider when choosing an anesthetic agent, the global warming potential of these inhaled agents, and more climate-friendly alternate techniques, also should be part of the decision-making process when possible.
Additionally, the amount of energy used to maintain safe, high-quality operating environments is multiple orders of magnitude more than what is required in routine clinical areas 56. Studies have shown that heating, ventilation, and air conditioning systems that provide air-quality control in operating rooms account for as much as 40% of total health care emissions 57. One option to decrease energy use is through heating, ventilation, and air conditioning setback systems that allow for less frequently used operating rooms to be maintained at less rigorous temperature and airflow standards while not in use (ie, overnight) 58.
Another way to improve sustainability within health care institutions is by reducing the use of disposable items. Although recycling is important, data show that items often are contaminated and can contain varying materials that are not all recyclable. This has the potential to make recycling of these products either impossible or technically difficult and very costly 53. Instead, making changes to practice and supplies by advocating for reusable items has the potential to make significant reductions in emissions. For example, a study assessing the carbon footprint of disposable compared with reusable specula at a U.S. academic hospital demonstrated that greenhouse gas emissions would be reduced by roughly 75% over a 1-year period by switching to metal specula 59.
Health care professionals have a moral obligation to patients and communities to advocate for environmentally responsible policies and practices at their institutions. It is important that ob-gyns educate themselves on these issues and advocate for institutional policies and guidelines that reduce and prevent unnecessarily high rates of greenhouse gas emissions in the operating room. See Box 4 for examples of opportunities to improve health care practice sustainability in obstetrics and gynecology.
Box 4.
Opportunities to Decrease the Carbon Footprint of Obstetrics and Gynecology
Remove unused supplies and downsize surgical and labor and delivery sterile fields.
Minimize opened materials and single-use devices.
Choose reusable instruments—steel trocars, metal speculums, reusable retractors, reprocessed energy devices.
Sort waste appropriately, limiting regulated medical waste to liquid blood and tissue.
Encourage the use of propofol over inhaled gases.
Power down equipment (HVAC setbacks, computers, lights, and camera boxes) when not in use.
Support breastfeeding and eliminate single-use formula feed plastic bottles.
Advocate for removing endocrine-disrupting chemicals from medical supplies.
Petition medical societies, policymakers, and regulatory agencies to follow evidence-based guidelines for reducing health care's carbon footprint and improving the health of patients.
HVAC, heating, ventilation, air conditioning.
Reprinted from Wright KN, Melnyk AI, Emont J, Van Dis J. Sustainability in obstetrics and gynecology. Obstet Gynecol 2023;142:1341–6. doi: 10.1097/AOG.0000000000005435. https://journals.lww.com/greenjournal/pages/articleviewer.aspx?year=2023&issue=12000&article=00010&type=Fulltext
Conclusion
As stated by the United Nations' International Court of Justice, climate change poses an “urgent and existential threat” to humankind ACOG recognizes and supports the gender diversity of all patients who seek obstetric and gynecologic care. In original portions of this document, authors seek to use gender-inclusive language or gender-neutral language. When describing research findings, this document uses gender terminology reported by investigators. To review ACOG's policy on inclusive language, see
https://www.acog.org/clinical-information/policy-and-position-statements/statements-of-policy/2022/inclusive-language
.Use of Language
Conflict of Interest Statement
All ACOG committee members and authors have submitted a conflict of interest disclosure statement related to this published product. Any potential conflicts have been considered and managed in accordance with ACOG's Conflict of Interest Disclosure Policy. The ACOG policies can be found on acog.org . For products jointly developed with other organizations, conflict of interest disclosures by representatives of the other organizations are addressed by those organizations. The American College of Obstetricians & Gynecologists has neither solicited nor accepted any commercial involvement in the development of the content of this published product.